

Abstract
Background
High-dose post-transplantation cyclophosphamide (PTC) has proven to be a valuable treatment modality for the prevention of graft-versus-host disease (GVHD) after stem cell transplant (SCT). Granulocyte colony stimulating factor (G-CSF) is routinely given after PTC to improve time to engraftment. Historically, based on the Johns Hopkins regimen, G-CSF is given on Day +5 post-SCT. However, this strategy has not been vigorously compared to other dosing strategies. We sought to assess the effect of delayed (Day +10) or omitted administration of G-CSF on various post-SCT outcomes.
Methods
Allogeneic SCT patients receiving PTC at standard dosing of 50 mg/kg daily on Days +3 and +4 were included in this retrospective analysis. G-CSF was given at the labeled dose of 5 mcg/kg (rounded to nearest vial) on Day +10 for 15 consecutive patients then omitted entirely for ten consecutive patients. These results were compared to historical controls that received G-CSF beginning Day +5 after PTC. All patients received antimicrobial prophylaxis with levofloxacin, acyclovir and posaconazole. The primary outcome was to determine time to engraftment defined, as an absolute neutrophil count ≥500, in each group. A complete list of secondary outcomes is below and includes febrile neutropenia and infection rates, incidence of acute GVHD, as well as survival and relapse rates.
Results
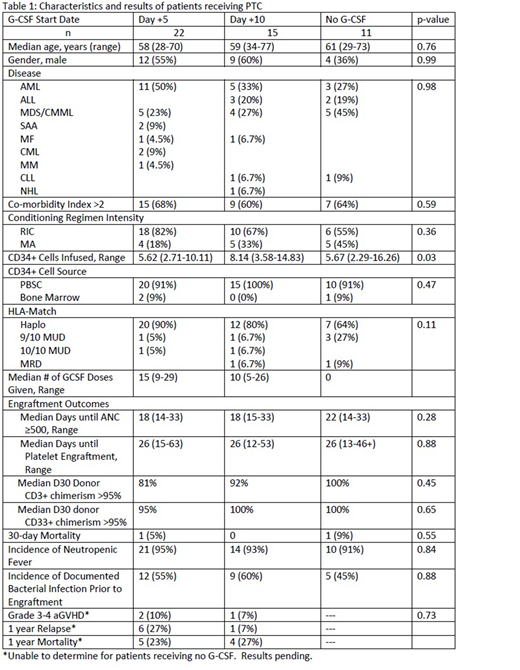
Forty-eight patients receiving PTC were included in the final analysis. Patient characteristics and outcomes are described in Table 1. There were no significant differences between the three groups with the exception of cells infused (p=0.03). While there was a longer time to ANC engraftment for patients not receiving GCSF after PTC, this was not statistically significant. Acute GVHD and first year outcomes were unable to be determined at this time for patients not receiving GCSF due to this population not reaching these endpoints at time of submission.
Conclusion
Administration of G-CSF after post transplant cyclophosphamide is not associated with earlier neutrophil engraftment. Secondary endpoints including platelet engraftment, aGVHD, incidence of febrile neutropenia, or infections were similar among all groups. A larger, randomized study is needed to confirm these results.
Bachier:Sanofi: Speakers Bureau; Seattle Genetics: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal